Hammer Toe Signs Symptoms
 Overview
Overview
A hammer toe can be defined as a condition that causes your toe to bend downward instead of pointing forward. While it can occur on any toe on your foot, it usually affects the second or third toe. If your baby toe curls instead of buckling, it is also considered a hammer toe. There are two types of hammer toes. If your toes still can move around at the joint, then it is considered a flexible hammer toe. It is a milder form of the condition and there are more treatment options. The other type is called a rigid hammertoes, which occurs when the tendons in your toe become so rigid that they push your toe joint out of alignment, and it cannot move at all. Typically, you will need surgery to fix it.
Causes
Medical problems, such as stroke or diabetes that affect the nerves, may also lead to hammertoe. For example, diabetes can result in poor circulation, especially in the feet. As a result, the person may not feel that their toes are bent into unnatural positions. The likelihood of developing hammertoe increases with age and may be affected by gender (more common in women) and toe length; for example, when the second toe is longer than the big toe, hammertoe is more likely to occur. Hammertoe may also be present at birth. Genetics may factor in to developing hammertoe, particularly if the foot is flat or has a high arch, resulting in instability.
{kind=link}
A toe stuck in an upside-down "V" is probably a hammertoe. Some symptoms are, pain at the top of the bent toe when putting on a shoe. Corns forming on the top of the toe joint. The toe joint swelling and taking on an angry red colour. Difficulty in moving the toe joint and pain when you try to so. Pain on the ball of the foot under the bent toe. Seek medical advice if your feet regularly hurt, you should see a doctor or podiatrist. If you have a hammertoe, you probably need medical attention. Ask your doctor for a referral to a podiatrist or foot surgeon. Act now, before the problem gets worse.
Diagnosis
Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred.
Non Surgical Treatment
Often padding and taping are the first steps in a treatment plan. Padding the hammer toe prominence minimizes pain and allows the patient to continue a normal, active life. Taping may change the imbalance around the toes and thus relieve the stress and pain. Anti-inflammatory drugs and cortisone injections can be prescribed to ease acute pain and inflammation caused by the joint deformity. Custom shoe inserts made by your podiatrist may be useful in controlling foot function. An orthotic device may reduce symptoms and prevent the worsening of the hammer toe deformity.
Surgical Treatment
Surgical Options: Several surgical procedures are available to the podiatric physician. For less severe deformities, the surgery will remove the bony prominence and restore normal alignment of the toe joint, thus relieving pain. Severe hammer toes, which are not fully reducible, may require more complex surgical procedures. Recuperation takes time, and some swelling and discomfort are common for several weeks following surgery. Any pain, however, is easily managed with medications prescribed by your podiatrist.
Bunions And High Heels
Overview
 A foot bunion is a common cause of foot pain caused by deformity of one of the toe bones. They most commonly affect the big toe, known as hallux abducto valgus, but can also affect the little toe, known as a bunionette. The classic presentation is a large bump on the outer side of the big toe that is red, swollen and painful caused by the toe deviating across towards the second toe. Left untreated, the condition usually gets gradually worse, so it is important to get treatment early on else you may end up needing bunion surgery.
A foot bunion is a common cause of foot pain caused by deformity of one of the toe bones. They most commonly affect the big toe, known as hallux abducto valgus, but can also affect the little toe, known as a bunionette. The classic presentation is a large bump on the outer side of the big toe that is red, swollen and painful caused by the toe deviating across towards the second toe. Left untreated, the condition usually gets gradually worse, so it is important to get treatment early on else you may end up needing bunion surgery.
Causes
Bunions are not inherited, but do tend to run in families. What is inherited is the poor or faulty foot type, that mechanically can lead to the instability around the joint that will eventually lead to bunions, how soon, how quickly and how bad they are or become is assumed to be very dependant on the footwear. A number of other factors are known to play a role in the cause of bunions and hallux valgus. Bunions can follow foot injuries and develop in those with neuromuscular problems. Those with flat feet or pronated feet appear to be more prone to the instability about the joint and have a higher incidence of bunions. Some activities (eg ballet dancing) puts added pressure on the joint and may increase the chance of bunions developing.
Symptoms
Bunions or hallux valgus tend to give pain predominantly from the metatarsal head on the inner border of the foot. The bunion tends to be painful mainly when in enclosed shoes and so is often more symptomatic in winter. As the front part of the foot splays and the great toe moves across towards the 2nd toe a bunion can also produce pain from the 2nd toe itself. The pain which a bunion produces on the 2nd toe is either due to direct rubbing between the great toe and the 2nd toe, a hammer toe type deformity produced due to crowding of the 2nd toe by the bunion and the 3rd toe.The hammer toe will either be painful from its top aspect where it rubs directly on shoe wear or its under surface in the area of the 2nd metatarsal head. This is made prominent and pushed to the sole of the foot by the 2nd toe rising upwards and driving the metatarsal head downwards.
Diagnosis
A doctor can very often diagnose a bunion by looking at it. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen.
Non Surgical Treatment
Wide toe box, bunion pads, orthotics, or a combination. Mild discomfort may lessen by wearing a shoe with a wide toe box or with stretchable material. If not, bunion pads purchased in most pharmacies can shield the painful area. Orthotics can also be prescribed to redistribute and relieve pressure from the affected articulation. If conservative therapy fails, surgery aimed at correcting abnormal bony alignments and restoring joint mobility should be considered. If the patient is unwilling to wear large, wider shoes to accommodate the bunion because they are unattractive, surgery can be considered; however, patients should be told that orthotic devices should be worn after surgery to reduce the risk of recurrence. For bursitis, bursal aspiration and injection of a corticosteroid are indicated. For osteoarthritic synovitis, oral NSAIDs or an intra-articular injection of a corticosteroid/anesthetic solution reduces symptoms. For hallux limitus or hallux rigidus, treatment aims to preserve joint mobility by using passive stretching exercises, which occasionally require injection of a local anesthetic to relieve muscle spasm. Sometimes surgical release of contractures is necessary. 
Surgical Treatment
Bunion surgery generally involves repositioning the maligned bones with a bone cut (osteotomy) and/or bone mending procedure (fusion). As such, the time it takes for bones to set or mend in the corrected position generally takes six weeks. Smokers and those in poor medical health may take longer to mend the bone. The biology of bone healing is about six weeks, that time frame can't be made quicker. What can be changed is the disability that one experiences while the bone is mending.
Does Overpronation Necessitate Surgery
Overview
Overpronation and underpronation describe general foot movements. These terms do not necessarily describe a medical problem with a foot. For example, you can overpronate and not have any problems or symptoms at all. It is important to have your foot structure and symptoms adequately assessed by your prescribing physician and a qualified practitioner such as a Canadian Certified Pedorthist. Once the underlying conditions and mechanical faults are assessed, an appropriate treatment plan including possible orthotic and footwear recommendations can be made.
Causes
Generally fallen arches are a condition inherited from one or both parents. In addition, age, obesity, and pregnancy cause our arches to collapse. Being in a job that requires long hours of standing and/or walking (e.g. teaching, retail, hospitality, building etc) contributes to this condition, especially when standing on hard surfaces like concrete floors. Last, but not least unsupportive footwear makes our feet roll in more than they should.
Symptoms
Because overpronation affects the entire lower leg, many injuries and conditions may develop and eventually cause problems not only in the leg and foot, but also the knee, hips and lower back. Pain often begins in the arch of the foot or the ankle. Blisters may develop on the instep, or on the inside edge of the heels. As overpronation continues and problems develop, pain will be felt elsewhere, depending on the injury.
Diagnosis
You can test for pronation by looking at the leg and foot from the back. Normally you can see the Achilles Tendon run straight down the leg into the heel. If the foot is pronated, the tendon will run straight down the leg, but when it lies on the heel it will twist outward. This makes the inner ankle bone much more prominent than the outer ankle bone.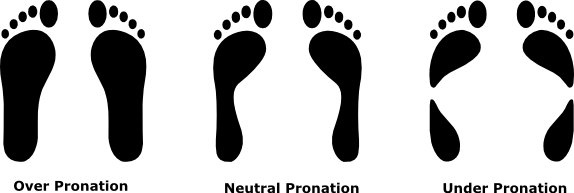
Non Surgical Treatment
When you see the doctor, he or she will likely perform a complete examination of your feet and watch you walk. The doctor will need to take x-rays to determine the cause of your flat feet. In some cases, further imaging may be needed, especially if your symptoms are severe and sudden in nature. Once you are properly diagnosed, your doctor will create an appropriate treatment plan. There are several options to correct overpronation, such as orthotics. In many cases, overpronation can be treated with non-surgical methods and over-the-counter orthotics. In severe cases, however, custom-made orthotics may work better. Orthotics provide arch support and therefore prevent collapse of the arch with weight bearing. They are made of materials such as spongy rubber or hard plastic. Your doctor will also want to examine your footwear to ensure they fit properly and offer enough medial support. Extra support and stability can be achieved with footwear that has a firm heel counter. If you are experiencing pain, you should be able to use over-the-counter pain medications such as ibuprofen to relieve symptoms.
Prevention
Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise.
Calf stretch:Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times.
Golf ball:While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds.
Big toe push: Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions.
Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times.
Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Overpronation and underpronation describe general foot movements. These terms do not necessarily describe a medical problem with a foot. For example, you can overpronate and not have any problems or symptoms at all. It is important to have your foot structure and symptoms adequately assessed by your prescribing physician and a qualified practitioner such as a Canadian Certified Pedorthist. Once the underlying conditions and mechanical faults are assessed, an appropriate treatment plan including possible orthotic and footwear recommendations can be made.
Causes
Generally fallen arches are a condition inherited from one or both parents. In addition, age, obesity, and pregnancy cause our arches to collapse. Being in a job that requires long hours of standing and/or walking (e.g. teaching, retail, hospitality, building etc) contributes to this condition, especially when standing on hard surfaces like concrete floors. Last, but not least unsupportive footwear makes our feet roll in more than they should.
Symptoms
Because overpronation affects the entire lower leg, many injuries and conditions may develop and eventually cause problems not only in the leg and foot, but also the knee, hips and lower back. Pain often begins in the arch of the foot or the ankle. Blisters may develop on the instep, or on the inside edge of the heels. As overpronation continues and problems develop, pain will be felt elsewhere, depending on the injury.
Diagnosis
You can test for pronation by looking at the leg and foot from the back. Normally you can see the Achilles Tendon run straight down the leg into the heel. If the foot is pronated, the tendon will run straight down the leg, but when it lies on the heel it will twist outward. This makes the inner ankle bone much more prominent than the outer ankle bone.
Non Surgical Treatment
When you see the doctor, he or she will likely perform a complete examination of your feet and watch you walk. The doctor will need to take x-rays to determine the cause of your flat feet. In some cases, further imaging may be needed, especially if your symptoms are severe and sudden in nature. Once you are properly diagnosed, your doctor will create an appropriate treatment plan. There are several options to correct overpronation, such as orthotics. In many cases, overpronation can be treated with non-surgical methods and over-the-counter orthotics. In severe cases, however, custom-made orthotics may work better. Orthotics provide arch support and therefore prevent collapse of the arch with weight bearing. They are made of materials such as spongy rubber or hard plastic. Your doctor will also want to examine your footwear to ensure they fit properly and offer enough medial support. Extra support and stability can be achieved with footwear that has a firm heel counter. If you are experiencing pain, you should be able to use over-the-counter pain medications such as ibuprofen to relieve symptoms.
Prevention
Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise.
Calf stretch:Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times.
Golf ball:While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds.
Big toe push: Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions.
Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times.
Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Physical Rehabilitation And Severs Disease
Overview
One of the more common limitations to children enjoying their youthful energy is Sever?s Disease. Sever?s Disease is a pathology that affects the heels of children in their high growth years (usually around 9-15), and it can be quite painful. It usually occurs due to repetitive trauma or impact at the heel. This means that if your child spends a lot of time running around (in sports, or just with friends) the continuous impact of his or her heel to the ground can cause this! Usually, most children will complain of heel pain specifically when they are active; these are considered milder cases. In more severe cases the pain may never cease, whether the child is active or not.
Causes
Sever?s disease is caused by repetitive tension and/or pressure on the growth center of the heel. Running and jumping place a large amount of pressure on the heels and can cause pain. Children with Sever?s may limp or have an altered gait due to the pain. Risk factors for Sever's include tight calf muscles, weak ankle muscles, and alignment abnormalities at the foot and ankle. Sever?s can also result from wearing shoes without sufficient heel padding or arch support.
Symptoms
In Sever?s disease, heel pain can be in one or both heels. It usually starts after a child begins a new sports season or a new sport. Your child may walk with a limp. The pain may increase when he or she stands on tiptoe. Your child?s heel may hurt if you squeeze both sides toward the very back. This is called the squeeze test. Your provider may also find that your child?s heel tendons have become tight.
Diagnosis
Sever condition is diagnosed by detecting the characteristic symptoms and signs above in the older children, particularly boys between 8 and 15 years of age. Sometimes X-ray testing can be helpful as it can occasionally demonstrate irregularity of the calcaneus bone at the point where the Achilles tendon attaches.
Non Surgical Treatment
Please realize that the disorder may last only a couple of weeks to as long as 1-2 years. The treatment plan as prescribed by your doctor MUST be adhered to closely, and the activity level of the child must be controlled during the early stages of treatment. All jumping and running sports, such as basketball, trampoline, volleyball, tennis, soccer, etc., must be eliminated as part of the initial treatment. Once the child has improved and the pain has subsided, a rigid stretching program must then be implemented.
Recovery
One of the most important things to know about Sever's disease is that, with proper care, the condition usually goes away within 2 weeks to 2 months and does not cause any problems later in life. The sooner Sever's disease is addressed, the quicker recovery is. Most kids can return to physical activity without any trouble once the pain and other symptoms go away.
One of the more common limitations to children enjoying their youthful energy is Sever?s Disease. Sever?s Disease is a pathology that affects the heels of children in their high growth years (usually around 9-15), and it can be quite painful. It usually occurs due to repetitive trauma or impact at the heel. This means that if your child spends a lot of time running around (in sports, or just with friends) the continuous impact of his or her heel to the ground can cause this! Usually, most children will complain of heel pain specifically when they are active; these are considered milder cases. In more severe cases the pain may never cease, whether the child is active or not.
Causes
Sever?s disease is caused by repetitive tension and/or pressure on the growth center of the heel. Running and jumping place a large amount of pressure on the heels and can cause pain. Children with Sever?s may limp or have an altered gait due to the pain. Risk factors for Sever's include tight calf muscles, weak ankle muscles, and alignment abnormalities at the foot and ankle. Sever?s can also result from wearing shoes without sufficient heel padding or arch support.
Symptoms
In Sever?s disease, heel pain can be in one or both heels. It usually starts after a child begins a new sports season or a new sport. Your child may walk with a limp. The pain may increase when he or she stands on tiptoe. Your child?s heel may hurt if you squeeze both sides toward the very back. This is called the squeeze test. Your provider may also find that your child?s heel tendons have become tight.
Diagnosis
Sever condition is diagnosed by detecting the characteristic symptoms and signs above in the older children, particularly boys between 8 and 15 years of age. Sometimes X-ray testing can be helpful as it can occasionally demonstrate irregularity of the calcaneus bone at the point where the Achilles tendon attaches.
Non Surgical Treatment
Please realize that the disorder may last only a couple of weeks to as long as 1-2 years. The treatment plan as prescribed by your doctor MUST be adhered to closely, and the activity level of the child must be controlled during the early stages of treatment. All jumping and running sports, such as basketball, trampoline, volleyball, tennis, soccer, etc., must be eliminated as part of the initial treatment. Once the child has improved and the pain has subsided, a rigid stretching program must then be implemented.
Recovery
One of the most important things to know about Sever's disease is that, with proper care, the condition usually goes away within 2 weeks to 2 months and does not cause any problems later in life. The sooner Sever's disease is addressed, the quicker recovery is. Most kids can return to physical activity without any trouble once the pain and other symptoms go away.
What Are Key Causes And Signs Of A Ruptured Achilles Tendon?
Overview
 An Achilles Tendon Rupture is a traumatic event that needs appropriate treatment by your physician. The rupture can either be partial or complete depending on the severity. A thorough evaluation needs to be made to differentiate a tendonitis from a rupture and to evaluate the extent of the rupture.
An Achilles Tendon Rupture is a traumatic event that needs appropriate treatment by your physician. The rupture can either be partial or complete depending on the severity. A thorough evaluation needs to be made to differentiate a tendonitis from a rupture and to evaluate the extent of the rupture.
Causes
Achilles tendon rupture occurs in people that engage in strenuous activity, who are usually sedentary and have weakened tendons, or in people who have had previous chronic injury to their Achilles tendons. Previous injury to the tendon can be caused by overuse, improper stretching habits, worn-out or improperly fitting shoes, or poor biomechanics (flat-feet). The risk of tendon rupture is also increased with the use of quinolone antibiotics (e.g. ciprofloxacin, Levaquin).
Symptoms
The pain from an Achilles tendon rupture is usually felt in the back of the lower leg, in the area 2 to 6 cm. above the Achilles tendon's attachment to the calcaneus. Individuals with an Achilles tendon rupture often describe a "pop" or similar feeling at the time of the injury. A "hole" or defect in the Achilles tendon can usually be felt under the skin in this area. A limp and inability to rise up on the toes of the affected foot are usually present. If the affected foot does not plantar flex when the calf muscles are squeezed an Achilles tendon rupture is very likely.
Diagnosis
Your doctor diagnoses the rupture based on symptoms, history of the injury and physical examination. Your doctor will gently squeeze the calf muscles, if the Achilles tendon is intact, there will be flexion movement of the foot, if it is ruptured, there will be no movement observed.
Non Surgical Treatment
As debilitating as they can be, the good news is that minor to moderate Achilles tendon injuries should heal on their own. You just need to give them time. To speed the healing, you can try the following. Rest your leg. Avoid putting weight on your leg as best you can. You may need crutches. Ice your leg. To reduce pain and swelling, ice your injury for 20 to 30 minutes, every three to four hours for two to three days, or until the pain is gone. Compress your leg. Use an elastic bandage around the lower leg and ankle to keep down swelling. Elevate your leg. Prop you leg up on a pillow when you're sitting or lying down. Take anti-inflammatory painkillers. Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (Advil, Motrin) and naproxen (Aleve) will help with pain and swelling. However, these drugs have side effects, such as an increased risk of bleeding and ulcers. They should be used only occasionally unless your health care provider says otherwise and should be taken with food. Check with your doctor before taking these if you have any allergies, medical problems or take any other medication. Use a heel lift. Your health care provider may recommend that you wear an insert in your shoe while you recover. It will help protect your Achilles tendon from further stretching. Practice stretching and strengthening exercises as recommended by your health care provider. Usually, these techniques will do the trick. But in severe cases of Achilles tendon injury, you may need a cast for six to 10 weeks or even surgery to repair the tendon or remove excess tissue. 
Surgical Treatment
While it is possible to treat an Achilles tendon rupture without surgery, this is not ideal since the maximum strength of the muscle and tendon rarely returns. The reason is the ends of the tendon are ruptured in a very irregular manner, almost like the ends of a paint brush. As soon as the tendon ruptures, the calf muscle (gastrocnemius muscle) continues to pull on the tendon and the end of the ruptured tendon pulls back into the leg, which is called retraction. Once the tendon retracts, it is never possible to get sufficient strength back without surgery, because the muscle no longer functions at the correct biomechanical length and is now stretched out. There are patients for whom surgery cannot be performed, in particular, due to existing medical conditions that may add to potential for complications following surgery. For these patients, a specially designed boot that positions the foot correctly and takes the pressure and tension off the muscle and tendon is used. Most importantly, a cast is never used because it causes permanent shrinkage (atrophy) of the calf muscle. The special boot permits pressure on the foot with walking. The boot also has a hinge to permit movement of the ankle. Many studies of Achilles tendon ruptures have shown that this movement of the foot in the boot while walking is ideal for tendon healing. If surgery is not recommended, it is essential to obtain special tests to check that the ends of the tendon are lying next to each other so that healing can occur. The best test to do this is an ultrasound and not an MRI.
Prevention
You can help to reduce your risk of an injury to your Achilles tendon by doing the following. When you start a new exercise regime, gradually increase the intensity and the length of time you spend being active. Warm up your muscles before you exercise and cool them down after you have finished. The benefit of stretching before or after exercise is unproven. However, it may help to stretch your calf muscles, which will help to lengthen your Achilles tendon, before you exercise. Wear appropriate and well-fitting shoes when you exercise.
Leg Length Discrepancy And Running
Overview
Leg length discrepancy is the difference in lengths of an individual?s legs. This difference may be anatomical or may be due to scoliosis, trauma/injury, arthritis, overpronation (collapse) of one foot, bowing of one leg or unequal bowing, surgery (hip or knee replacement), pelvic tilting or ageing. The difference can also be functional caused by differing forces of the soft tissues, such as weakness in muscle tissue on one side, or a weakness/tightness in joint tissue. A difference in leg lengths also results when running on indoor banked tracks, beaches and banked streets and side walks (for drainage). Many people have a measurable difference in their leg lengths which is compensated for by their bodies. As we age this compensation does not work as well. An x-ray and physical measurements will define the discrepancy and the adjustment needed.
Causes
LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio.
Symptoms
Often there are few or no symptoms prior to the age of 25-35. The most common symptom is chronic lower back pain, but also is frequently middle and upper back pain. Same-sided and repeated injury or pain to the hip, knee and/or ankle is also a hallmark of a long-standing untreated LLD. It is not uncommon to have buttock or radiating hip pain that is non-dermatomal (not from a disc) and tends to go away when lying down.
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
After the leg length discrepancy has been identified it can be categorized in as structural or functional and appropriate remedial action can be instigated. This may involve heel lifters or orthotics being used to level up the difference. The treatment of LLD depends on the symptoms being experienced. Where the body is naturally compensating for the LLD (and the patient is in no discomfort), further rectifying action may cause adverse effects to the biomechanical mechanism of the body causing further injury. In cases of functional asymmetry regular orthotics can be used to correct the geometry of the foot and ground contact. In structural asymmetry cases heel lifts may be used to compensate for the anatomic discrepancy.

Surgical Treatment
Shortening techniques can be used after skeletal maturity to achieve leg length equality. Shortening can be done in the proximal femur using a blade plate or hip screw, in the mid-diaphysis of the femur using a closed intramedullary (IM) technique, or in the tibia. Shortening is an accurate technique and involves a much shorter convalescence than lengthening techniques. Quadriceps weakness may occur with femoral shortenings, especially if a mid-diaphyseal shortening of greater than 10% is done. If the femoral shortening is done proximally, no significant weakness should result. Tibial shortening can be done, but there may be a residual bulkiness to the leg, and risks of nonunion and compartment syndrome are higher. If a tibial shortening is done, shortening over an IM nail and prophylactic compartment release are recommended. We limit the use of shortenings to 4 to 5 cm leg length inequality in patients who are skeletally mature.
Leg length discrepancy is the difference in lengths of an individual?s legs. This difference may be anatomical or may be due to scoliosis, trauma/injury, arthritis, overpronation (collapse) of one foot, bowing of one leg or unequal bowing, surgery (hip or knee replacement), pelvic tilting or ageing. The difference can also be functional caused by differing forces of the soft tissues, such as weakness in muscle tissue on one side, or a weakness/tightness in joint tissue. A difference in leg lengths also results when running on indoor banked tracks, beaches and banked streets and side walks (for drainage). Many people have a measurable difference in their leg lengths which is compensated for by their bodies. As we age this compensation does not work as well. An x-ray and physical measurements will define the discrepancy and the adjustment needed.
Causes
LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio.
Symptoms
Often there are few or no symptoms prior to the age of 25-35. The most common symptom is chronic lower back pain, but also is frequently middle and upper back pain. Same-sided and repeated injury or pain to the hip, knee and/or ankle is also a hallmark of a long-standing untreated LLD. It is not uncommon to have buttock or radiating hip pain that is non-dermatomal (not from a disc) and tends to go away when lying down.
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
After the leg length discrepancy has been identified it can be categorized in as structural or functional and appropriate remedial action can be instigated. This may involve heel lifters or orthotics being used to level up the difference. The treatment of LLD depends on the symptoms being experienced. Where the body is naturally compensating for the LLD (and the patient is in no discomfort), further rectifying action may cause adverse effects to the biomechanical mechanism of the body causing further injury. In cases of functional asymmetry regular orthotics can be used to correct the geometry of the foot and ground contact. In structural asymmetry cases heel lifts may be used to compensate for the anatomic discrepancy.
Surgical Treatment
Shortening techniques can be used after skeletal maturity to achieve leg length equality. Shortening can be done in the proximal femur using a blade plate or hip screw, in the mid-diaphysis of the femur using a closed intramedullary (IM) technique, or in the tibia. Shortening is an accurate technique and involves a much shorter convalescence than lengthening techniques. Quadriceps weakness may occur with femoral shortenings, especially if a mid-diaphyseal shortening of greater than 10% is done. If the femoral shortening is done proximally, no significant weakness should result. Tibial shortening can be done, but there may be a residual bulkiness to the leg, and risks of nonunion and compartment syndrome are higher. If a tibial shortening is done, shortening over an IM nail and prophylactic compartment release are recommended. We limit the use of shortenings to 4 to 5 cm leg length inequality in patients who are skeletally mature.
The Cause For Posterior Tibial Tendon Dysfunction (PTTD)
Overview
Tendons do a lot of work. In fact, a great deal of what happens when you walk can be related to tendons tugging and pulling in appropriate ways in their proper places. With this in mind, it?s hardly surprising that on occasion, (probably because we too often forget to send them ?Thank you? cards), tendons may decide that they?ve had it. They may buck their responsibilities, shirk their work, and in all other ways cease to function properly. And that may mean bad news for you. Take the posterior tibial tendon: it runs from the bottom of the calf, goes right under that bump on the inside of the ankle (the medial malleolus) and ends up attaching itself to a bone on the inside of the middle of your foot (the navicular bone). It?s the main tendon that keeps the arch of your foot in place, and it helps a bunch in walking, too. Over time, though, we tend to put a lot of stress on this faithful tendon, especially if we?ve put on extra weight, or do a lot of activities that stress it out, walking, running, hiking, or climbing stairs. Sometimes athletes (who do a lot of that walking and running stuff) may put so much stress on the tendon that it tears suddenly. But for many of us, damage may take place gradually (i.e. the tendon stretches out) until the tendon tells us that it flat out quits. (It sometimes doesn?t even give two weeks notice.) In short, you may develop posterior tibial tendon dysfunction (PTTD). 
Causes
There are numerous causes of acquired adult flatfoot, including fracture or dislocation, tendon laceration, tarsal coalition, arthritis, neuroarthropathy, neurologic weakness, and iatrogenic causes. The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
There are four stages of adult-acquired flatfoot deformity (AAFD). The severity of the deformity determines your stage. For example, Stage I means there is a flatfoot position but without deformity. Pain and swelling from tendinitis is common in this stage. Stage II there is a change in the foot alignment. This means a deformity is starting to develop. The physician can still move the bones back into place manually (passively). Stage III adult-acquired flatfoot deformity (AAFD) tells us there is a fixed deformity. This means the ankle is stiff or rigid and doesn???t move beyond a neutral (midline) position. Stage IV is characterized by deformity in the foot and the ankle. The deformity may be flexible or fixed. The joints often show signs of degenerative joint disease (arthritis).
Non surgical Treatment
Conservative treatment also depends on the stage of the disease. Early on, the pain and swelling with no deformity can be treated with rest, ice, compression, elevation and non-steroidal anti-inflammatory medication. Usually OTC orthotic inserts are recommended with stability oriented athletic shoes. If this fails or the condition is more advanced, immobilization in a rigid walking boot is recommended. This rests the tendon and protects it from further irritation, attenuation, or tearing. If symptoms are greatly improved or eliminated then the patient may return to a supportive shoe. To protect the patient from reoccurrence, different types of devices are recommended. The most common device is orthotics. Usually custom-made orthotics are preferable to OTC. They are reserved for early staged PTTD. Advanced stages may require a more aggressive type orthotic or an AFO (ankle-foot orthosis). There are different types of AFO's. One type has a double-upright/stirrup attached to a footplate. Another is a gauntlet-type with a custom plastic interior surrounded be a lace-up leather exterior. Both require the use of a bulky type athletic or orthopedic shoes. Patient compliance is always challenging with these larger braces and shoes. 
Surgical Treatment
Surgery should only be done if the pain does not get better after a few months of conservative treatment. The type of surgery depends on the stage of the PTTD disease. It it also dictated by where tendonitis is located and how much the tendon is damaged. Surgical reconstruction can be extremely complex. Some of the common surgeries include. Tenosynovectomy, removing the inflamed tendon sheath around the PTT. Tendon Transfer, to augment the function of the diseased posterior tibial tendon with a neighbouring tendon. Calcaneo-osteotomy, sometimes the heel bone needs to be corrected to get a better heel bone alignment. Fusion of the Joints, if osteoarthritis of the foot has set in, fusion of the joints may be necessary.